Conduction Recovery is More Likely in Patients With Late vs. Early Pacemaker Implant Following TAVR
 Author: Maher Bazzi, MD, MSE, Additional Authors**
Author: Maher Bazzi, MD, MSE, Additional Authors**
Background
High degree AV block leading to pacemaker (PPM) implant remains the most frequent complication following transcatheter aortic valve replacement (TAVR). The likelihood of PPM implant is reported to be ~ 11-14%. Although most AV block requiring PPM implant occurs within the first 48 hours (“early”), a significant minority of patients develops high degree AV block after 48 hours (“late”), and typically after discharge. There is limited data on how often AV nodal conduction recovers after PPM implant and whether “early” vs. “late“ implant post TAVR makes a difference.
Objective
The goal of this study is to determine the incidence of AV nodal conduction recovery in patients who underwent PPM implant and to identify characteristics that may predict conduction recovery. Moreover, we set out to ascertain whether AV nodal conduction is more likely to recover in patients who have “early” vs “late” AV block leading to PPM implant.
Methods
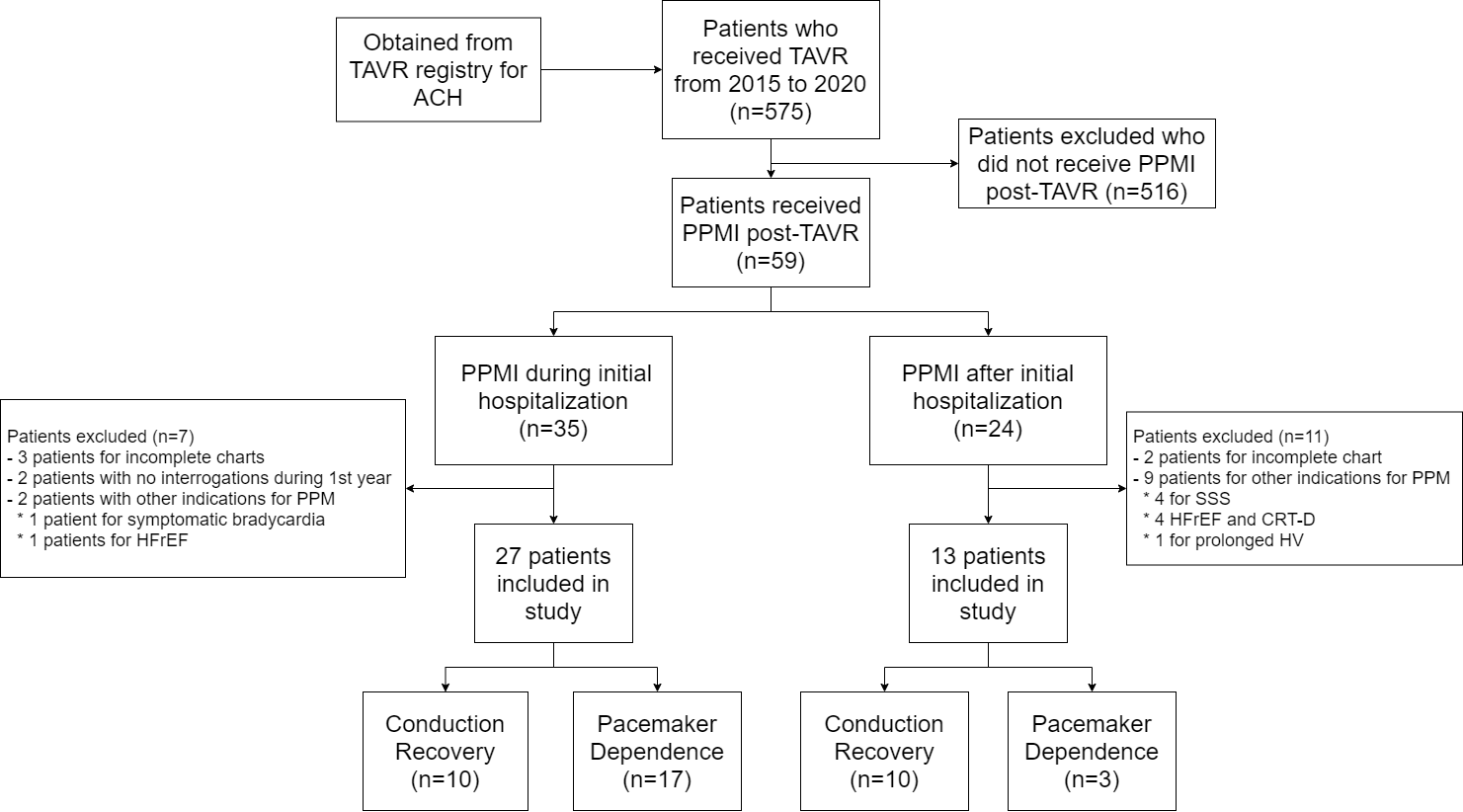
In this observational study, we reviewed all TAVR cases performed between 2015 and 2020 at Summa’s Akron City Hospital. We identified all patients that required subsequent PPM implant and we further divided patients into those that developed AV block requiring a PPM implant within 48 hours (“early”), and those that developed it after 48 hours (“late” and after discharge). We performed a retrospective chart review, collected baseline characteristics including pre-TAVR and post-TAVR EKGs, and analyzed PPM interrogations performed thereafter up to one year. As recent papers offer no consensus on the exact definition of conduction recovery, we chose <30% ventricular pacing as the cut-off to describe conduction recovery.
Results
Of 575 patients who underwent TAVR, 40 patients (6.9%) developed AV block requiring a PPM. Of those, 27 patients (67.5%) developed AV block within 48 hours while 13 patients developed AV block > 48 hours and needed readmission for PPM implant. Surprisingly, 20 of 40 (50%) of patient had AV nodal conduction recovery. Ten of 27 (37%) patients with “early” PPM implant versus 10 of 13 (77%) patients with “late” PPM implant had AV nodal conduction recovery (p-value of 0.0183). Furthermore, the presence of permanent atrial fibrillation, sinus bradycardia or first-degree AV block pre-TAVR were associated with a higher likelihood of permanent pacemaker dependency.
Conclusion
In this large observational study 50% of all patients who developed AV block requiring PPM implant had recovery of AV nodal conduction. In addition, patients presenting with AV block after discharge (> 48 hours post procedure) showed a greater likelihood of AV nodal conduction recovery. These findings suggest that AV block post TAVR may often be related to inflammation and edema rather than permanent scarring.
**Additional Authors:
Maher Bazzi, MD, MSE, Summa Health Heart and Vascular Institute, Akron, OH
Ottorino Costantini, MD, Summa Health Heart and Vascular Institute, Akron, OH