Constricted No More
Author: Peter Hu, MD*
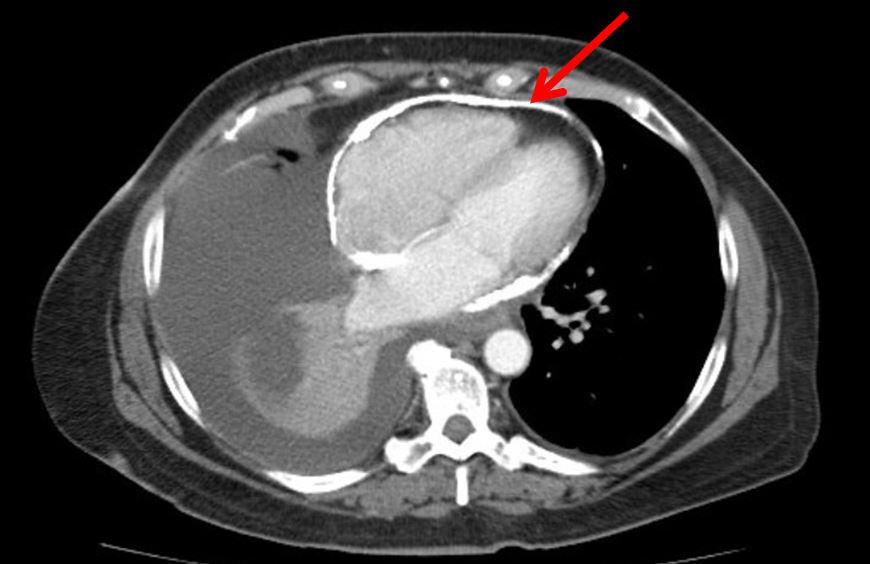
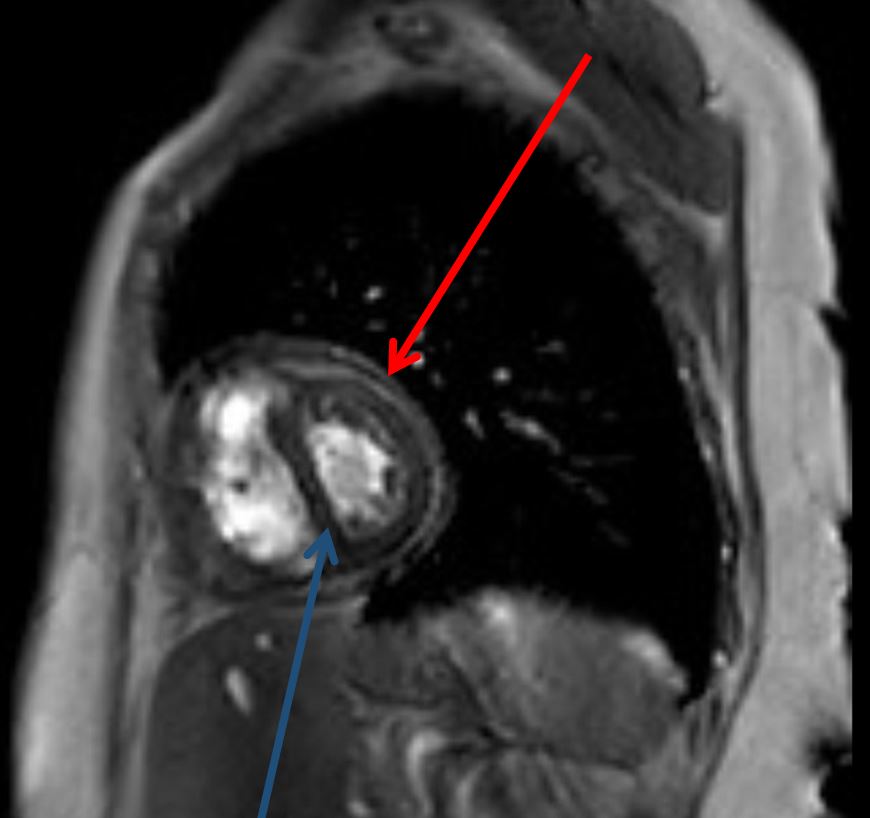
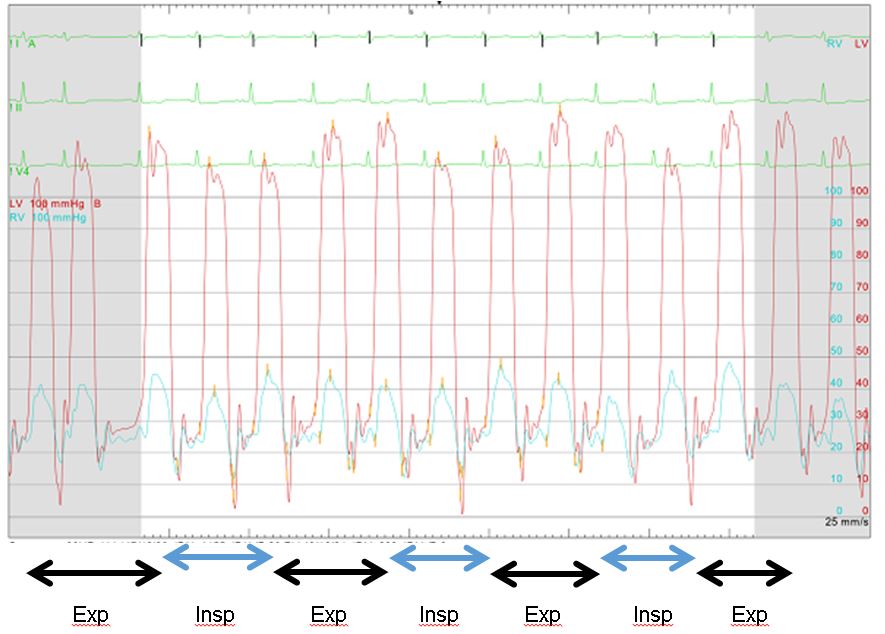
A 58-year old woman was admitted to the hospital for further evaluation of a recurrent right-sided, exudative pleural effusion requiring three prior therapeutic thoracenteses in the past month. She had no history of malignancy, radiation exposure, or recent infectious symptoms. Echocardiogram demonstrated a calcified pericardium with septal bowing into the left ventricle during inspiration. CT chest demonstrated a moderate right-sided pleural effusion with circumferential pericardial calcification. Cardiac MRI showed similar circumferential pericardial thickening with respirophasic variation of the interventricular septum consistent with constrictive physiology. Simultaneous right and left heart catheterization showed elevated and equal right and left ventricular diastolic pressure tracings as well as respirophasic discordance between the right and left ventricular systolic pressures.
She was started on an oral diuretic and underwent pericardiectomy one-month later. Pathology was consistent with marked fibrous thickening of the fibrosa layer of the pericardium with mild chronic inflammation and no signs of acute inflammation, malignancy, or caseating necrosis. Ultimately, no definitive cause of the patient’s constrictive pericarditis was identified. The patient is doing well since her surgery with her postoperative echocardiogram showing normal left ventricular and right ventricular function following pericardiectomy.
Constrictive pericarditis must be recognized through a combination of patient symptomatology, signs on physical exam, EKG, imaging findings, and invasive hemodynamics. Common imaging findings include pericardial thickening with or without calcification and evidence of heart failure. The hallmark of constriction is ventricular interdependence and dissociation of intracardiac and intrathoracic pressures. For patients with newly diagnosed constriction without evidence of hemodynamic compromise or chronic constriction, a trial of diuretics can be considered. Ultimately, pericardiectomy is the only definitive treatment for patients with chronic, symptomatic constrictive pericarditis who fail medical therapy.


* Cleveland Clinic, 9500 Euclid Ave, Rm J3-129, Cleveland, OH 44195